Scaling Beyond the Sandbox: A Pragmatic Blueprint for AI in Healthcare (Part 2)
- Corey Mercy
- 2 days ago
- 3 min read

It is relatively easy to make an artificial intelligence tool look like a miracle worker inside a controlled environment. When you are operating within a dedicated clinical innovation hub, utilizing isolated, de-identified datasets, the integration challenges are minimized, the stakes are managed, and the outcomes feel predictable.
But as any veteran technology executive knows, the real test begins when you pull down the partition walls and attempt to hook that algorithm into the central nervous system of a living, breathing healthcare enterprise.
In my years directing IT strategy, enterprise applications, and revenue cycle networks across sprawling clinical ecosystems, I learned that healthcare delivery systems are inherently resistant to sudden, uncoordinated shocks. A hospital or public health agency is a complex web of legacy databases, deeply entrenched clinical habits, and continuous compliance mandates. If your strategy for scaling AI relies on clinicians shifting their workflows to fit a new tool, your deployment is dead on arrival. To scale successfully, the technology must quietly bend to the operational realities of the floor.
The first major hurdle in moving from pilot to production is the structural friction of our data architecture.
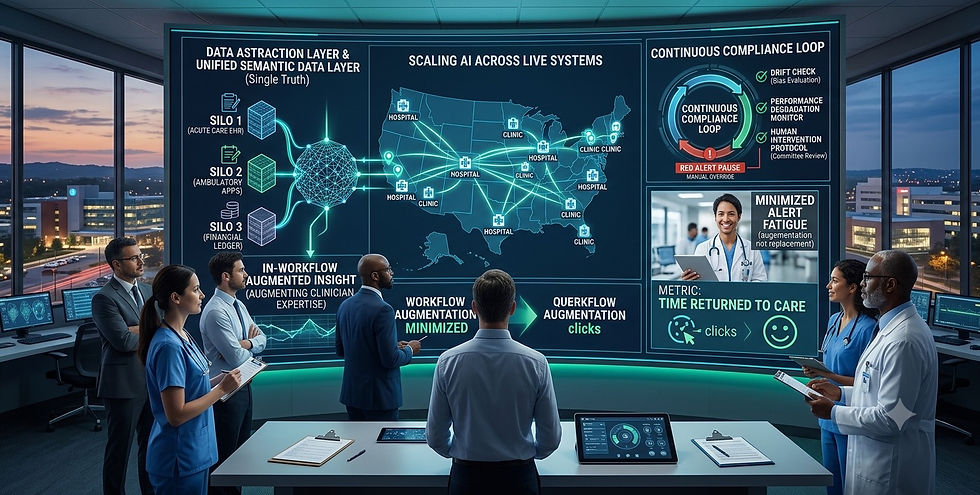
True clinical intelligence requires a continuous, real-time understanding of the patient journey. Yet, in most healthcare delivery environments, that data is locked behind silos—trapped between electronic health records, ancillary clinical application streams, and ERP platforms. If you train an AI model using clean, curated data in a sandbox, it will inevitably stutter when confronted with the messy, disjointed data pipelines of a live health care ecosystem.
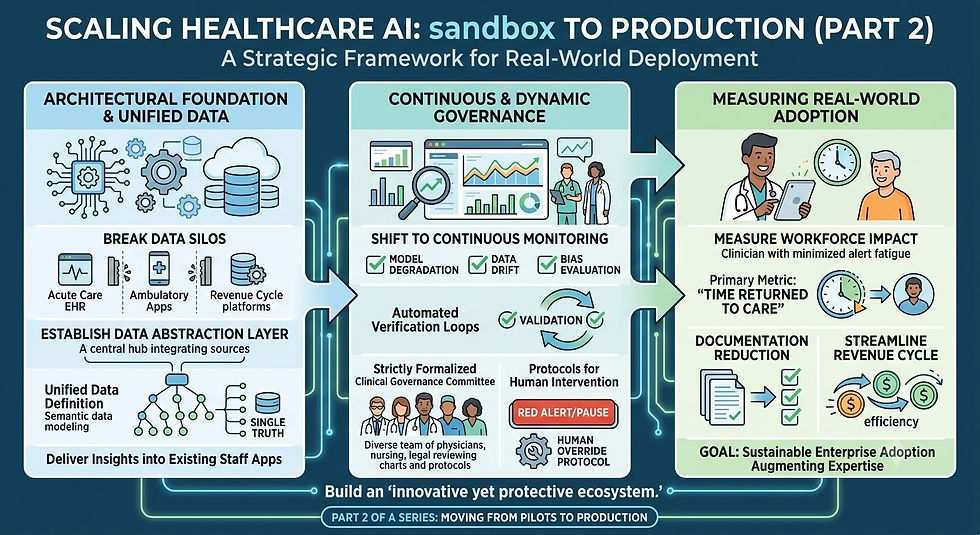
Before scaling an AI tool across multiple clinics or public health divisions, you must establish an underlying data abstraction layer. This is where semantic data modeling transitions from a validation tool into an operational anchor. By creating an interconnected semantic data layer that unifies disparate data definitions across your clinical and administrative applications, you give your AI tools a single, trustworthy version of truth. It allows the technology to ingest data from legacy databases and modern cloud frameworks seamlessly, delivering insights directly into the tools and dashboards your staff already open every single morning.
The second hurdle is the shift from static compliance to continuous, dynamic governance.
When you are managing a pilot, certifying regulatory alignment with frameworks like HIPAA, GDPR or the NIST AI Risk Management Framework is a milestone you achieve before launch. When you scale to enterprise production, compliance becomes a living, real-time requirement. Models degrade. Data drift occurs as clinical demographics shift, and an algorithm that demonstrated high clinical efficacy in month one can develop blind spots by month six.
Building a sustainable AI governance framework means establishing automated verification loops. You need technical monitoring systems that constantly evaluate model inputs and outputs for variance, bias, or performance degradation. Just as importantly, you must formalize clinical governance committees. These committees are made up of physicians, nursing staff, informatics analysts, and legal counsel who review performance logs regularly. If an algorithm’s recommendation deviates from established clinical baselines, there must be an actionable, clear protocol for human intervention.
Finally, scaling successfully demands that we measure what actually matters. Far too often, IT initiatives fail because leadership measures technical metrics like processing speed or algorithmic precision, while the front-line staff is drowning in alert fatigue. If a new AI-driven tool adds three extra clicks to a nurse's documentation workflow, it doesn't matter how accurate the backend model is…it will be rejected.
To turn early optimization wins into sustainable enterprise adoption, focus your scaling metrics on time returned to care. Does this deployment reduce the burden of documentation? Does it streamline the revenue cycle verification backlog? Does it allow a clinician to look at their patient instead of a monitor?
By anchoring your scaling strategy in architectural discipline, continuous data integrity, and a deep respect for the clinical workflow, you can successfully move AI out of the sandbox and build an enterprise ecosystem that is both rapidly innovative and fiercely protective of patient trust.
Comments